She was also struggling with withdrawal from heroin. An acquaintance who was working as a sex worker recommended she call the man she worked for.
The man picked her up at the Quality Dairy at Pennsylvania Avenue and Kalamazoo Street and took her back to his apartment. He provided her with heroin.
“That was the beginning of slavery for me,” she said. The man advertised her for sexual services on BackPage.com and expected her to see as many as 15 clients a day. When the Internet trade was slow, he would have her walk Kalamazoo to find clients. He would bundle her and other women off to other cities to perform as well. He paid her solely in heroin.
Nearly a year later, she met Dr. Paul DeWeese when her pimp — wanting her to clean up her act so she could have his child — took her to him for addiction treatment. She poured her heart out to DeWeese.
“He got silent,” she said. “Then he said, ‘You have to get out of there.’”
The two hatched a plot for her to escape, with his assistance.
She said DeWeese “saved me.”
But now, the state of Michigan has suspended DeWeese’s medical license amid ongoing federal and state probes over the former state lawmaker’s prescribing practices.
With DeWeese’s help, she located a doctor over an hour away who is willing to continue her treatment. Unlike DeWeese, though, the doctor doesn’t accept Medicaid, meaning she will have to foot the bill in order to continue on buprenorphine, which dulls heroin withdrawal.
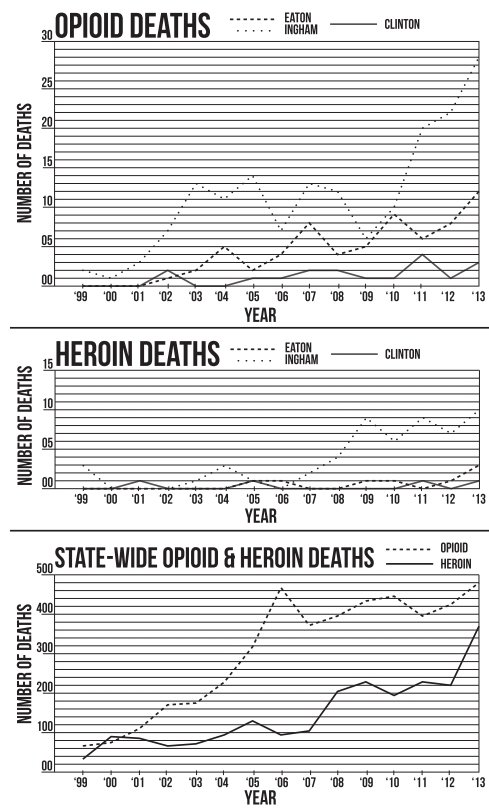
For Cassandra (not her real name), expensive and inconvenient as it may be, medical treatment may well save her life. Heroin is killing people locally and statewide at an alarming rate. (See chart.)
In Lansing, seven people have died from heroin overdoes so far this year, compared to three in all of last year and one in 2013, according to the Police Department. Overdoses have risen to 47 this year, compared to 26 in the previous two years combined. Chief Mike Yankowski called it an "epidemic."
Dr. Robert Townsend runs Denali Healthcare, which has clinics all over the state of Michigan, including one on Michigan Avenue that opened this year. The clinic specializes in chronic pain management.
As a matter of course, he said, he also addresses opioid addiction. He said he knows the pain patients face when a doctor who has been providing care for pain suddenly can’t assist anymore.
“Many times a physician will treat someone with a shortacting opioid — like Narco,” Townsend said. “But as the patient develops tolerance and needs more and more, the physician grows concerned and cuts them off. Where do the patients have left to go?”
When a patient is suddenly cut off by a primary care physician, he said, many people turn to street pharmacies. Prescription opioid pills sold on the street can fetch as much as a dollar a milligram, quickly putting them out of reach of most opioid dependent people.
Heroin is the cheapest alternative out on the street, much of it coming from Latin American cartels.
Data from state health officials as well as from the Ingham County Health Department show that indeed opioid and heroin-related deaths are a growing problem.
“Heroin use is a significant problem,” said Linda Vail, chief health officer for Ingham County. “In the first four months of 2014, there were two heroin overdose deaths. In the first four months of 2015, there were 10 heroin overdose deaths. This is a five-fold increase.”
And those numbers for deaths could have been even higher. Vail said emergency responders have used a drug called Narcan to stop overdoses in the county.
“Local EMS administered Narcan 68 times from January 1 to June 30 in 2014,” Vail said. “In 2015 in that same 6-month period, they administered it 132 times.”
“Michigan is a high-prescribing state,” Vail added. “In 2012, there were 107 painkiller prescriptions for every 100 people. For comparison, Illinois had 68 for every 100 people.”
Narco and other drugs like it, Townsend said, are short acting and short-term pain medications. To effectively use such prescriptions in treatment of chronic pain, he said, the drug would have to be taken six or seven times a day.
Townsend said the answer in good chronic pain management is not necessarily an end to pain for the patient, but rather a reduction so they can resume normal life activities. He uses buprenorphine for most pain patients. Buprenorphine is a drug used to treat opioid addiction, but can be addictive itself. The drug is less potent than methadone, according to the federal Substance Abuse and Mental Health Services Administration website.
The issue becomes one of perception when it comes to pain management Townsend said.
Most people after an injury think, “Am I in pain today? Do I need to take medications for it?” while others fall into a “very subtle” way of thinking which leads to dependence.
“I need to take the medicine because I might hurt,” Townsend said the subtle thinking goes.
The problem of prescription opioid addiction and abuse as well as heroin is being taken seriously by top politicians. Lt. Gov. Brian Calley is leading a statewide working group trying to devise ways to help people with chronic pain, but also to address prescription drug abuse, diversion of drugs from prescriptions and heroin use.
“If the report [from the Calley working group] shows that there are policy and law changes that will assist in addressing this problem, I’d be more than happy to put it on the fast track,” said Sen. Rick Jones, R-Grand Ledge, chairman of the Judiciary Committee.
All of this, however, leaves former patients of DeWeese scrambling to line up new pain management or addiction treatment.
Jacob Burns, 36, has struggled with serious back-related pain since 2007. He rattles off a list of back issues from sciatica to herniated discs.
“It was hard to get the chronic pain treated,” Burns said. “Doctors don’t want to take the risks.”
He ultimately landed in DeWeese’s clinic in January. Contrary to what the FBI affidavit used to secure a federal subpoena alleges, Burns said DeWeese was by the books in his care.
“He made me bring in all my medical records,” the father of three said. “He made me get a new MRI.”
Without DeWeese, Burns is getting some help from readicare clinics. He’s unsuccessfully tried emergency rooms to get help from local emergency rooms.
“All his patients are left hanging,” he said. “None of the local hospitals will help us.”





Support City Pulse - Donate Today!
Comments
No comments on this item Please log in to comment by clicking here